
A Clinical Case Of Stent Implantation Into The Area Of The Myocardial Bridge
- Article
- Article Info
- Author Info
Background
The Myocardial bridges in the human heart are a benign developmental anomaly that can lead to acute myocardial ischemia [1-4]. According to a number of authors, muscle bridges are often determined in the region of the anterior interventricular artery, while the diameter of the coronary artery before the bridge is larger than after it. In the area of the bridge, the tunica intima of the artery has a normal thickness, proximal to it, it underwent hyperplasia until the development of the atherosclerotic process [5]. Ishikawa notes the unlikely likelihood of atherosclerotic lesions of the intima of arterial segments intersected by myocardial bridges [6].
Bockeria et al. emphasize the histological similarity of myocardial bridges with the myocardial tissue of other parts of the heart [5]. Such anomalies of the blood vessels of the heart cause impaired blood flow, and, therefore, a decrease in blood pressure in the area distal to the bridge, which can cause damage to the inner lining of the vessel and increase the length of the atherosclerotic plaque. Atherosclerotic lesion of the coronary arteries results in a narrowing of their lumen and a deterioration in the blood supply to the myocardium. Most often, congenital anomalies of the coronary arteries are not dangerous, but pathological processes in them can lead to the development of myocardial infarction. The severity of coronary obstruction due to a myocardial bridge depends on factors such as the location, thickness, extent of the muscular bridge, and the state of myocardial contractile function.
One of the important studies of myocardial bridges, which is the gold standard in the diagnosis of myocardial bridges, is coronary angiography. It provides an opportunity to visualize the internal contours of the coronary arteries and allows you to assess the degree and extent of stenosis and, often, to determine the causes of its occurrence. Angiographic signs of the myocardial bridge are recognized: a) – curvature of the segment of the affected coronary artery; b) – uniform narrowing of the vessel lumen by more than 40% in systole and restoration of the diameter in diastole (systolic narrowing); c) – clear signs of narrowing in at least two angiographic projections, in which the percentage of narrowing is greatest, and the part of the vessel distal to the bridge is free from compression; d) absence of vascular compression caused by pharmacological agents or catheter [7-14].
Aim
The aim of our study was to demonstrate a rare case of coronary artery stent placement in the area of the myocardial bridge Patient G., male. born in 1967, does not smoke, does not drink alcohol, has not previously taken medications was admitted to Grodno Regional Clinical Cardiology Center with clinical signs of acute coronary syndrome with ST segment elevation along the anterior wall of the left ventricle.
Method
At the pre-hospital stage, the ambulance team performed thrombolysis-actilize. Biochemical blood test was done upon admission-
Aspartate aminotransferase 253 U / L ((0-40) U / L)
Alanine aminotransferase 61 U / L ((0-41) U / L)
Creatine kinase 4110 U / L ((38-174) U / L)
MB fraction of creatine kinase 460 U / L ((0-25) U / L)
Troponin I 50,000 ((0-20))
At the clinic, coronary angiography was performed: at the border of anterior third and middle third, the branch is S-shaped, twisted with the presence of a myocardial bridge with almost complete overlap of the lumen in systole (Figure 1) and restoration of the diameter in diastole (Figure 2) – systolic narrowing.

Figure 1: The complete overlap of the lumen in systole.,/a>
Figure 2: The restoration of the diameter in diastole – systolic narrowing.
At the time of coronary angiography, pain in the region of the heart does not bother, hemodynamic parameters are without negative dynamics. After 12 hours, the patient resumed pain in the area of the heart of angina pectoris and negative dynamics on the ECG. A decision was made to perform a repeat coronary angiography with the determination of further treatment tactics for the patient. Due to the deterioration of the general condition of the patient, coronary angiography was performed, followed by implantation of a stent into the area of the myocardial bridge (Figure 3 and 4). “Abbott BMW Universal II” coronary guide-wire was used for stent implantation. During the operation was established stent “Meril BioMime” 2.75x19mm 18 atm. Introduced “Omnipack 350” 150 ml, Heparin 18000 U, Nitroglycerin intracoronary – 900 mcg.
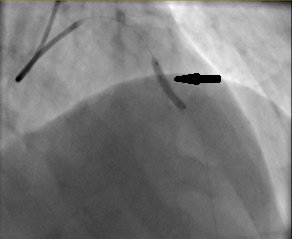
Figure 3: The process of stent implantation in the area of the myocardial bridge.
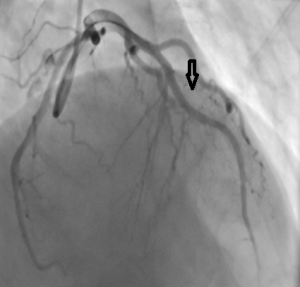
Figure 4: The stent located into the area of the myocardial bridge.
In order to prevent thrombotic complications in the postoperative period, the appointment is indicated as Aspicard 75 mg per day and Clopidogrel 75 mg per day; For the prevention of peptic ulcer, Omeprazole 20 mg per day; In order to correct dyslipidemia, Lipromak 20 mg per day; and in order to correct heart rate and blood pressure, Bisoprolol 2.5 mg in the morning and Ramipril 5 mg in the morning.
A repeated biochemical blood test indicates a positive dynamics of acute phase biochemical parameters.
Aspartate aminotransferase 275 U / L ((0-40) U / L)
Alanine aminotransferase 58 U / L ((0-41) U / L)
Creatine kinase 2107 U / L ((38-174) U / L)
MB fraction of creatine kinase 152 U / L ((0-25) U / L)
Lactate dehydrogenase 1629 e / l ((207-414) U / l)
Troponin test on the 7th day: Troponin I 594 ((0-20)
Result
The patient’s state of health after the surgical treatment has improved, pain in the heart area does not bother, hemodynamic parameters are normal, the ECG shows positive dynamics – the ST segment drops below the isoline with the formation of a negative T wave. In choosing the treatment of the myocardial bridge, drug therapy is preferred, but in patient’s refractory to pharmacotherapy, surgical dissection of muscle bridges, coronary artery bypass grafting and stenting of this segment of the coronary artery are used. Indications for stenting or surgical treatment in the presence of a clinically significant myocardial bridge can be presented when clinical manifestations of myocardial ischemia are proven. For this, stress tests, stress echocardiography, 24-hour ECG monitoring and radioisotope methods with physical activity are used.
Conclusion
Patients should be under medical supervision, since under certain conditions the presence of a myocardial bridge can cause sudden death, Thus, the data of the world literature and data in our clinic indicate that myocardial muscle bridges, previously considered a “harmless” congenital anomaly of the coronary arteries, can cause the development of acute coronary syndrome up to the development of acute myocardial infarction and cause disability of the working population.
References
1.Starodubov OD, Efremova OA (2016) Miokardial’nye myshechnye mostiki: patofiziologicheskie osobennosti i kliniko-morfologicheskie priznaki. Nauchnye vedomosti Belgorodskogo gosudarstvennogo universiteta. Medicina Farmacija :15-21.
2.Medushevskaja JuA (2017) Osobennosti stroenija i gemodinamiki vetvej venechnyh arterij, raspolozhennyh pod myshechnymi mostikami. Vesennie anatomicheskie chtenija: sbornik statej nauch.-prakt. konf., posvjashhennoj pamjati docenta D. D. Smirnova. Grodno :115-118.
3.Shheglova EV, Chotchaeva ZH, Andrejuk VA, Gol’tjapin DB (2013) Miokardial’nye mosty kak prichina ishemii miokarda. Vestnik molodogo uchenogo 2: 42-45.
4.Loukas M (2011) Myocardial bridges: a review. Clin Anat 24: 675-683.
5.Bokerija, LA, Bokerija OL, Mozhina AA, Tetvadze IV (2010) Miokardial’nye myshechnye mostiki. Jembriologija, anatomija, patofiziologija: Literaturnyj obzor. Chast’ I. Bjulleten’ NCSSH imeni A.N. Bakuleva RAMN 11: 62-71.
6.Ishikawa Y (2009) Anatomic properties of myocardial bridge predisposing to myocardial infarction. Circulation 120: 376-383.
7.Belov JuV, Bogopol’skaja OM (2004) Miokardial’nyj mostik – vrozhdennaja anomalija koronarnogo rusla. Kardiologija 12: 89-94.
8.Angelini P, Velasco JA, Flamm S(2002) Coronary anomalies. Incidence, pathophysiology, and clinical relevance. Circulation 105: 2449-24
9.HG Klues, ER Schwarz, J vom Dahl, T Reffelmann,H Reul, et al. (1997) Disturbed intracoronary hemodynamics in myocardial bridging: early normalization by intracoronary stent placement. Circulation 96: 2905-2913.
10.Ferreira AG (1991) Myocardial bridges: morphological and functional aspects. Br Heart J 66: 364-367.
11.Bahaaldin A (2018) Do not miss the bridge. Thorac Cardiovasc Surg 156: 1627-1628.
12.PB Villela, Gláucia MM (2019) A New Marker of Myocardial Bridge? Arq Bras Cardiol 112: 18-19.
13.Raouf M, Hatem K, Jacques N, Fabien P, Bernhard M (2019) Myocardial bridging: a contemporary review. Rev Med Suisse 15: 1232-1238.
Yuri AF, Yukio I,Tetuo M,Yoshikiyo A,Toshiharu I (2018) Settlement of stenotic site and enhancement of risk factor load for atherosclerosis in left anterior descending coronary artery by myocardial bridge. Arterioscler Thromb Vasc Biol 38: 1407-1414.
*Corresponding author: Ivantsov AU, Department of Normal Anatomy Grodno State Medical University, Republic of Belarus.
Citation: Ivantsov AU, Tsydzik IS, Ivantsou UA (2021) A Clinical Case Of Stent Implantation Into The Area Of The Myocardial Bridge. Arch Resp Res 2: 003.
Received: Mar 30, 2021; Accepted: May 17, 2021; Published: May 25, 2021
Copyright: © 2021 Ivantsov AU et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits un-restricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
1Department of Normal Anatomy Grodno State Medical University, Republic of Belarus
2Grodno Regional Clinical Cardiology Center, Republic of Belarus
3Department of Traumatology, Grodno State Medical University, Republic of Belarus
Citation: Ivantsov AU, Tsydzik IS, Ivantsou UA (2021) A Clinical Case Of Stent Implantation Into The Area Of The Myocardial Bridge. Arch Resp Res 2: 003.
Received: Mar 30, 2021; Accepted: May 17, 2021; Published: May 25, 2021
Copyright: © 2021 Ivantsov AU et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits un-restricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding Authors:
Ivantsov AU, Department of Normal Anatomy Grodno State Medical University, Republic of Belarus.
